Depending on what is found, you may be:
- Given medications and be followed up regularly
- Referred to an interventional cardiologist for an transcatheter valve treatment (e.g. TAVI/TAVR transcatheter aortic valve implantation/replacement or Mitraclip repair)
- Referred to a cardiac surgeon for possible valve surgery (open heart surgery – conventional/minimally invasive)
Your heart valve specialist team (Surgeon/Cardiologist) will:
- Explain which therapy may be the best option for your condition
- Explain the different ways of treating the valves
- Explain the risks, benefits and possible complications
- Describe the procedure
- Explain the post-procedure care
- Answer your questions and clarify your doubts
- Help you reach a decision and set a date for the surgery
Heart Valve Surgery
There are four valves in your heart made of thin and strong flaps of tissue that open and close as your heart pumps to make sure that blood flows in the right direction through your heart. However, valve problems may occur either because of a birth defect, or ageing, or even from certain diseases.
Your damaged valves can either be repaired or replaced through a heart valve surgery.
Your surgeon will always try to save as much of your valve as possible unless this affects the result of the surgery. If the repair fails, he will replace the valve at the same operation.
Valves can be replaced by:
- Mechanical Valves
- Artificial manufactured valves
- Lasts a long time
- Risk of a blood clot forming, so you will need to take blood thinning drugs (anticoagulants)
- Bioprosthetic valves (pig or cow tissue) and Allograft valves (human valve tissue)
- You will probably not need to take anticoagulants except for the first few weeks after the surgery.
- May require surgery every 10-15 years as they wear out faster
There are a few methods for heart valve surgery:
- Surgical
- An incision will be made down the middle of your chest.
- Your breastbone is separated.
- You will be placed on a heart-lung machine
- Minimally invasive surgery
- "Keyhole surgery"
- Operations is performed through small incisions.
- Special instruments are passed through and the surgeon uses a video monitor to see the inside of your chest.
How should you prepare for the surgery?
- You should stop smoking at least four weeks before surgery to enable a faster recovery and to reduce the risk of complications. You should also consider stopping smoking for good.
- You should eat a healthy balanced diet and rest well before the surgery.
What happens during the surgery?
Before the surgery:
- All the necessary tests (e.g. blood tests, X-ray etc) will be done two weeks before your admission to hospital.
- In this way, you will only need to be admitted the day before the surgery, helping you to save on your hospital bill.
- Should any of your tests be abnormal, you can be treated in time so as not to delay surgery.
- You will be admitted on the day before the surgery- A team of doctors will check you to make sure that everything is in order.
- They will explain the surgery and other details to you again. You can address any further concerns with them.
- You will visit the Cardiac Surgery Intensive Care Unit (CTICU) where the nurse will explain to you what to expect after the surgery.
- The anaesthetist will visit you and explain the anaesthetic procedure.
- You will be given a mild sedative to help you sleep that night.
- You will not be allowed to eat or drink after midnight.
On the day of the surgery:
- Further sedation will be given in the morning just before the operation.
- An antibacterial soap will be used to clean you the night before and in the morning of the surgery to reduce the risk of wound infection.
After the surgery:
- The surgery will usually take between three to five hours after which, you will be looked after in the CTICU for one to two days.
- The chest tubes and urinary catheter will be removed and you will be transferred to the ward.
- You will stay for another three to four days before discharge.
- Total recovery usually takes four to six weeks.
- You will be given follow-up dates to see your surgeon - at the second week after the operation.
- Your surgeon may want to see you more frequently if there is a need.
- At the same time, you will also be seen by your family doctor and cardiologist.
What are the potential risks or complications?
Complications are not common, but some can be serious.
- If you are receiving valves made from animal tissue, these valves may develop calcium deposits over time which may hamper the valve's function. When this happens, the valve will have to be replaced.
- Blood clots may develop on the surface of the substitute valve. When these blood clots dislodge, they may get wedged in an artery. However, this can be treated with drugs or surgery.
- There is a risk of infection of the heart muscle, but this can be treated with intravenous antibiotics.
TAVI / TAVR (Transcatheter Aortic Valve Implantation also known as Transcatheter Aortic Valve Replacement)
Why is Transcatheter Aortic Valve Implantation (TAVI) needed?
TAVI is used to treat severe aortic stenosis, a condition in which the aortic valve becomes narrowed, obstructing the outflow of blood from the heart and thereby requiring the heart to work harder to pump blood around the body.
TAVI is a procedure performed using the Edwards Sapien Transcatheter Heart Valve (THV), an artificial heart valve designed to be inserted into your heart so that it holds open and replaces your diseased aortic valve. It consists of a metal stent (made of steel or cobalt-chromium) which secures the device in its intended position inside your own valve, and valve leaflets (made of biological material derived from cows) to direct the flow of blood out of your heart.
TAVI now offers effective treatment to patients who are at high risk for conventional open heart surgery. It is also intended to prevent further damage to the heart from aortic stenosis and to prolong life, which medical therapy cannot do.
What can I expect before the procedure?
Before the procedure, you will undergo routine investigations to evaluate whether TAVI is possible,and which of the two techniques for TAVI (Transfemoral or Transapical route) is most appropriate for you. The investigations will also identify any other considerations that need to be addressed for your treatment.
The investigations include:
- A physical examination
- Angiogram
- Blood tests
- Chest X-ray
- CT Scans
- Electrocardiogram
Two approaches of TAVI
Whether you are selected to undergo the transfemoral or the transapical approach, this procedure will be performed under general anesthesia. As the heart is not opened to expose the aortic valve, fluoroscopy (X-rays) and transesophageal echocardiography (ultrasound) are used to visualise the heart and THV, and to guide the insertion of the THV. The duration of X-ray exposure that you will receive will normally be less than 30 minutes, the normal length of time it takes for a coronary artery procedure in the cardiac catheterisation laboratory.
Transfemoral TAVI
The transfemoral device is designed to be implanted through the blood vessel (femoral artery) in your leg. Due to the size of the catheter (hollow tube) being placed in your artery for this approach, your doctors will evaluate the angiograms and/or CT scans to ensure that your blood vessels are big enough for this device. Prior to implantation, the THV is “crimped” (carefully compressed to a size that fits inside your femoral artery) using a specifically designed crimping device. The crimped THV is mounted onto a balloon delivery catheter, a special device used to carry the THV up to the heart and directly into your aortic valve. The valve is then expanded using a balloon to fit inside your stenotic aortic valve, holding your own valve open permanently. Once the valve is in position and the delivery system is removed from your femoral artery, the artery is closed using a special suture device designed for this purpose. After the procedure, you will be transferred to the Coronary Care Unit (CCU).
Transapical TAVI
The transapical approach is used for patients whose arteries are too small or too diseased for the transfemoral approach.
The delivery system for this approach is designed for THV implantation through the tip (apex) of your heart, which is reached through a small incision made between the ribs just below the left nipple. The crimped THV and delivery system is inserted through the apex of your heart directly into your stenotic aortic valve. The valve is then expanded using a balloon to fit across your stenotic aortic valve, holding it open permanently. After the procedure, you will be transferred to the Cardiothoracic Intensive Care Unit (CTICU).
What happens after the procedure?
After the TAVI procedure, you will be transferred to either the CCU ward or the CTICU ward for close monitoring. When you are first transferred, you may be under sedation and on ventilatory support. Over the course of the next 24 hours, you will be awakened from the sedation and allowed to breathe on your own with the ventilation tube removed. You will remain in the CCU or CTICU ward until your doctor feels that you can be transferred to a regular hospital ward, where you will continue to be monitored until your discharge from the hospital, usually within 5 – 7 days.
You will be given blood thinning medications such as aspirin and clopidogrel (Plavix). You should continue taking these or other blood thinners for 6 months after the procedure, and aspirin for life (as recommended for routine stenting of coronary blood vessels and any replacement heart valve). The following routine checks will be completed while you are in hospital.
- A physical examination
- Chest X-ray
- Daily electrocardiogram (ECG)
- Standard blood tests
- Transthoracic echocardiogram (TTE)
Thereafter, you will be required to see your doctor in the clinic after 30 days, 6 months, 12 months, and then once a year. The routine checks such as echocardiography are repeated at your first and subsequent outpatient follow-ups.
What are the potential risks/complications of the procedure?
Like any other operations, there are risks associated with this procedure. However, the long-term risk to your life and your quality of life may be higher if severe Aortic Stenosis is not treated.
The risks of TAVI include the following:
- Death (1 – 10%)
- Heart or blood vessel injury, such as perforation or damage of blood vessels, heart muscle valve structures that may require emergency surgery (1 – 10%)
- Heart attack (1 – 10%)
- Stroke (1 – 10%)
- Clot (1 – 10%)
- Hemorrhage (bleeding) requiring transfusion (0.1 – 5%)
- Hematoma (1 – 10%)
- Hypertension (high blood pressure) / Hypotension (low blood pressure) (0.1 – 5%)
- Kidney failure needing dialysis (0.1 – 10%)
- Kidney dysfunction (0.1 – 25%) – Allergic dye reaction (0.1 – 1%)
- Anesthesia reaction (1 – 10%)
- Abnormal heart rhythms (0.1 – 25%)
- Heart conduction system injury, which may require a permanent pacemaker (1 – 10%)
- Fever (0.01 – 1%)
- Infection including valve infection (0.01 – 1%)
- Pericardial effusion / cardiac tamponade (bleeding into the heart sac) (0.1 – 1%)
- Nerve injury (0.01 – 0.1%)
- Arteriovenous (AV) fistula an abnormal passageway between an artery and a vein) (0.01 – 0.1%)
- Short term use of intra-aortic balloon pump to assist heart function (1%)
- Lower limb ischemia / limb loss (0.5%)
- Emergency aortic valve surgery by conventional method (1 – 3%)
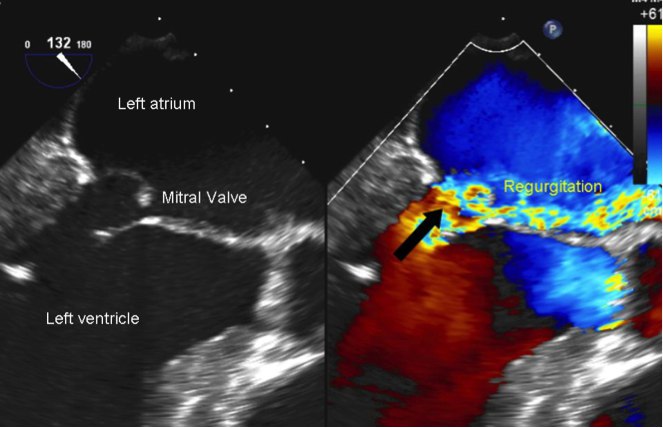
MitraClip Therapy for Mitral Regurgitation
The mitral valve is located between the two chambers on the left side of the heart which directs blood flow in one direction - from the upper chamber (left atrium) to the lower chamber (left ventricle). When this valve does not close completely, mitral valve regurgitation or backflow of blood in the left ventricle occurs. In severe cases, reduced blood flow is pumped out of the heart. This creates excessive workload on the heart leading to dilation of the heart chambers. If left untreated, it can result in heart failure.
There are currently several options of treatment available for Mitral Valve Regurgitation. These include medical treatment, surgery, or less invasive valve repair such as the mitraclip therapy.
What can I expect before the procedure?
Some investigations would need to be performed before the procedure. These include but are not limited to a transthoracic and transesophageal echocardiogram (ultrasound test for the heart). These two tests will allow for more accurate assessment of the mitral valve to determine if mitraclip therapy is suitable. Other tests such as coronary angiograms, electrocardiograms, chest X-rays and blood tests may also be needed prior to the procedure.
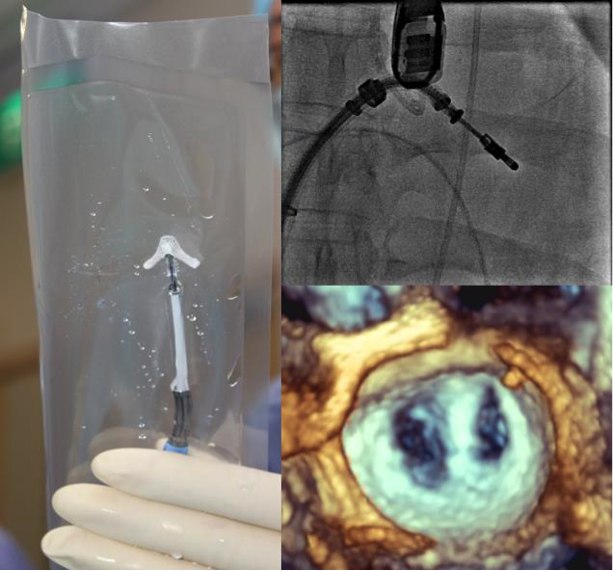
The Procedure
The mitraclip therapy procedure is done under general anesthesia and takes approximately 3 to 4 hours. A catheter (long thin flexible tube) is guided through the femoral (leg) vein to reach the heart. The clip is delivered through the catheter to the region of the mitral valve. Upon reaching the mitral valve, it clips the mitral valve to allow it to close better. The clip is left on the mitral valve while the rest of the delivery system and the catheter are removed.
What happens after the procedure?
After mitraclip therapy procedure, you will be transferred to the cardiac monitoring unit for a day. After this, your cardiologist would review you and may transfer you to the regular hospital ward for the next two days before discharge. Additional tests would be performed after the mitraclip therapy procedure. These include a repeat transthoracic echocardiogram, blood tests and a chest X-ray. You may also be given blood thinners such as aspirin and or clopidogrel for six months.
