The oesophagus or gullet (食道 in Mandarin) is a muscular tube which carries food from the mouth into the stomach. Once food enters the oesophagus, it is then moved down through a series of muscular contractions called ‘peristalsis’.
When food passes from the lower end of the oesophagus into the stomach, it encounters a special muscular ring known as the lower oesophageal sphincter (LES). When the LES relaxes, the food will enter the stomach. The LES is important because it prevents back flow of food and acid from the stomach into the oesophagus.
However, when the LES fails to relax, the food in the oesophagus is unable to enter the stomach. Over time, the motor function of the oesophageal muscle weakens and the oesophagus enlarges. This inability of the oesophagus to relax known as Achalasia.
Achalasia is a relatively rare disease affecting about 1 in 100,000 people. It occurs in both adults and children, with men and women being equally affected. The exact cause of it is unknown.
Achalasia is a chronic disease. Most people suffering from this condition have difficulty in swallowing and make dietary adjustments such as eating in small portions or choosing a liquid diet. Some may become thin and malnourished and suffer a diminished quality of life. Nevertheless, this condition is treatable. Speak to your doctor for further details.
What are the signs & symptoms of Achalasia?
Difficulty swallowing
Food regurgitation
Coughing at night
Aspiration
Recurrent lung infections
Chest pain
Weight loss
How is Achalasia diagnosed?
An upper endoscopy is a common test used to examine the upper digestive tract. The procedure is usually performed in an outpatient setting. It involves the insertion of an endoscope, which is a thin flexible tube with a camera at the tip, to allow for a visual examination of the oesophagus and stomach. The procedure takes less than 10 minutes and is often performed under light sedation. It is very useful for excluding any tumour or blockage of the oesophagus. In Achalasia, the oesophagus will be wider than usual, and is sometimes filled with residual food (Fig. 1a and Fig. 1b).
Fig. 1aFig. 1b
Another method of detection is using barium, a common X-ray contrast liquid. When it is swallowed, barium will outline the inner surface of the oesophagus, allowing the oesophagus to be seen on X-ray. The typical features of Achalasia include a dilated oesophagus and narrowing at the end of the oesophagus, producing a ‘bird beak’ appearance.
Oesophageal manometry is the most important test to confirm the diagnosis of Achalasia, and allows us to see what happens when a patient swallows. A small thin tube with pressure sensors is inserted gently into the oesophagus and stomach. The movement of the oesophagus and pressure of the LES will be recorded to determine any impairment in function.
What are the treatment options for Achalasia?
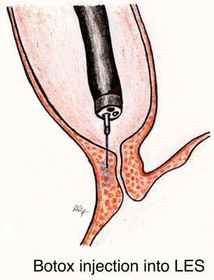
Botulinum Toxin Injection
Commonly known as Botox, a Botulinum Toxin Injection blocks the release of chemicals in the muscle which induces contractions, hence resulting in relaxation of the LES. It is a safe and effective treatment for Achalasia. Side-effects are minimal but relief is temporary.
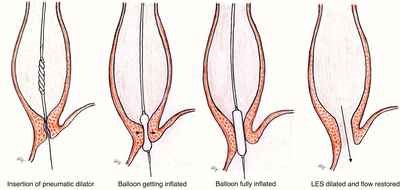
Balloon Dilatation
A balloon attached to the tip of a catheter is inserted into the lower oesophagus. On inflation of the balloon, the force will enlarge the passage of the lower oesophagus into the stomach. The LES pressure will be reduced as the force tears the muscle fibres of the sphincter.
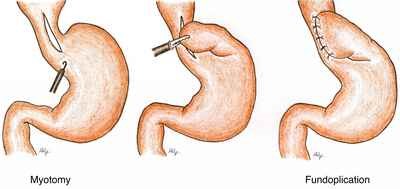
Laparoscopic Myotomy
This involves surgical division of the muscle of the LES. This procedure is done under general anaesthesia. It is a minimally invasive surgery where the muscle fibres of the LES are cut longitudinally from the lower oesophagus to upper gastric (cardia).
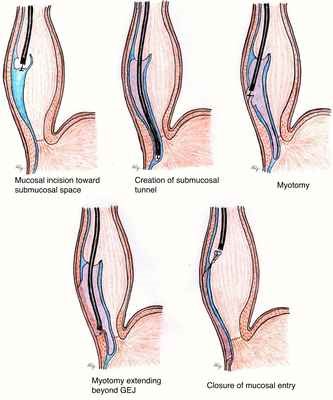
Peroral Endoscopic Myotomy (POEM)
This is the treatment for Achalasia with no surgical incision required. The procedure is done endoscopically under general anaesthesia. The endoscope is inserted into the oesophageal lumen. A tunnel is created below the inner lining of the oesophagus all the way to the LES. The muscle fibres of the lower oesophagus and gastric cardia are then divided endoscopically.
Endoscopic view of POEM
A: 2cm longitudinal incision is made. B: Submucosal tunnel is created leaving the underlying muscularis propria. C: Circular muscle is cut, preserving the outer longitudinal muscle layer. D: Clips are placed to close the initial mucosal layer.
Find A Doctor
Click here to access our Find A Doctor directory for a list of doctors treating this condition across our NUHS institutions.